“At Malik’s Multispeciality Dental Clinic, our procedures and treatments are tailored to match the specific concerns of each and every member of your family from the perspective your entire mouth being healthy.”

MINOR ORAL SURGERY PROCEDURES
- Quick Links
- Surgical extraction of tooth/teeth
- Multiple extraction
- Difficult extractions /medically compromised patients
- Surgical management of impacted teeth
- Surgical endodontics(apicectomy/ root resection/ root amputation)
SURGICAL EXTRACTION OF TOOTH/TEETH /MULTIPLE EXTRACTION DIFFICULT EXTRACTIONS /MEDICALLY COMPROMISED PATIENTS
May be required when there are
- Retained roots, which cannot be grasped by the forceps
- Previous history of difficult or attempted and failed extraction technique
- Previous history of difficult or attempted and failed extraction technique
- Any large restoration with root canal therapy—brittle teeth
- Hypercementosis/ankylosis of a tooth
- Germinated/dilacerated tooth
- Radiographic evidence of complicated/difficult root pattern
- Sclerosis of the bone
- Teeth associated with pathology—periapical granuloma, cyst, tumour, etc
- Impacted teeth, embedded teeth

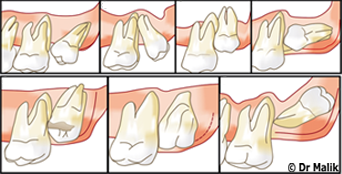
SURGICAL MANAGEMENT OF IMPACTED TEETH

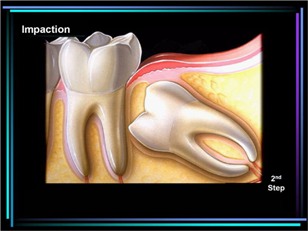
An impacted tooth may be
- An unerupted tooth that is in the process of eruption and is not likely to erupt based on clinical and radiographic findings
- Malposed tooth /erupted or unerupted which is in an abnormal position in the maxilla or in the mandible
- An embedded or impacted tooth—is the tooth that has failed to erupt completely or partially to its correct position in the dental arch and its eruption potential
Indications For Removal Of Impacted Teeth
- Recurrent pericoronitis/pain/infection/caries—pericoronitis is the inflammation of the gingiva surrounding a crown of a partially erupted tooth
- Deep periodontal pocket associated with partially erupted tooth
- Prior to orthodontic treatment—to control the tooth crowding in the mandible
- Prevention of root resorption and caries—caries of the impacted tooth crown and the adjacent tooth can be seen due to an inability to access and clean the area. Root resorption of the distal root of the adjacent second molar is seen in the 21 to 30 years of age group. Root resorption of lateral incisor may be seen associated with an impacted maxillary or man dibular canine
- Management of cysts and tumours, abscess
- Prevention of pathological fractures
- Before the fabrication of dentures, impacted teeth should be removed
- Prophylactic removal

SURGICAL ENDODONTICS(APICECTOMY/ROOT RESECTION/ROOT AMPUTATION)
Apicoectomy, apical surgery, endodontic surgery, root resection, roots amputation are the terms which are used for surgery involving the root apex to treat the apical infection. It is the cutting off of the apical portion of the root and curettage of periapical necrotic, granulomatous, inflammatory or cystic lesions. In spite of good endodontic treatment, if periapical lesions are not resolved, then apical surgery is undertaken.

MAJOR ORAL AND MAXILLOFACIAL PROCEDURES
- Quick Links
- <Back to Minor Oral Surgery Procedures>
- Orofacial and Neck Infections and their Management
- Trauma / fracture of the maxilla/mandible due to injury or road traffic accidents
- Temporomandibular Joint Disorders
- Orthognatic surgery
- Preprosthetic Surgery
- Diseases of the Salivary Glands
- Facial Neuropathology/Orofacial Region Pain
- Sensory Disturbances of Face and Jaws
- Surgical correction of cleft lip and palate
- Oral Malignancies
OROFACIAL AND NECK INFECTIONS AND THEIR MANAGEMENT
The majority of infections in orofacial and neck region belong to this group. Infections arise within jaw bones, and can be classified as those arising from:
(i)Pulp disease(ii)Periodontal disease(iii)Secondary infection from a cyst (Iv)Remaining root fragment (v) Residual infection (vi) Pericoronal infection.
These manifests in the following forms:
(i)Periapicalabscess (ii)Periodontal abcess (iii)Infected cyst
(iv) Residual abscess (v) Pericoronal abscess.
- Traumatic: Occasionally, trauma from penetrating wounds of soft and hard tissues of the face can lead to orofacial infection.
- Implant surgery
- Reconstructive surgery
- Infections arising from contaminated needle punctures.
- Others: arising from other factors such as infected sinus, salivary gland afflictions, etc.
- Secondary to oral malignancies.
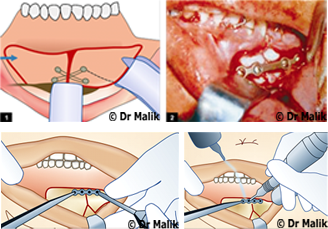
Surgical Therapy- Incision and Drainage of an Abscess
The abscess is drained surgically and simultaneously dental treatment is also done. It involves the blunt exploration of the entire anatomic space or the abscess cavity; with the opening up of all the tissue planes within the abscess cavity. The abscess cavity is then irrigated with betadine and saline solution. A drain is inserted into the depth of the space.

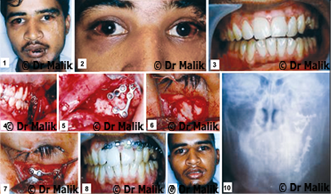
TRAUMA / FRACTURE OF THE MAXILLA(UPPER JAW)/MANDIBLE(LOWER JAW) DUE TO INJURY OR ROAD TRAFFIC ACCIDENTS
The conservative treatment
Reduction and fixation of the fractured mid face is indicated in cases, where surgery is not possible on account of poor general condition of the patient It may be used also as a supplementary measure with the surgical treatment of midfacial fracture.
Supervised spontaneous healing:
In such cases the progress of healing is supervised. The patient is advised to avoid chewing during the first 2 to 3 weeks and should remain on a liquid or semisolid diet.
Monomaxillary fixation:
This method is used when tooth bearing section of the upper jaw is not fractured and therefore can serve as fixation point. The arch bar or palatal acrylic plates can be used. This can be used for unilateral fractures of maxilla or higher fractures without occlusal discrepancies. As a rule monomaxillary fixation must be maintained for six weeks.
Intermaxillary fixation (IMF):
Intermaxillary fixation is maintained for 3 to 4 weeks and at the end of this period IMF wires and the lower arch bars are removed.
Open Reduction
Open reduction is carried out under general anaesthesia with nasal intubation.
Fracture of the Floor of the Orbit (eye) (Blow-out Fracture)
Treatment consists of surgical exploration of orbital floor and reconstruction of the orbital floor by silastic sheet or bone graft whenever necessary. Otherwise balloon support or ribbon gauze packing can be used in the maxillary sinus.
Treatment of Fractures of the Zygomatic Bone (upper jaw)
In majority of cases early operation is advisable, provided that there are no ophthalmic or cranial complications. Open reduction may be required and transosseous wiring and bone plating.
Fractures of the Nasal Bone
Incidence of nasal fracture is quite high, because of the prominent position of the nose. Nasal fracture is usually the result of direct injury; it can occur as an isolated fracture or it may be combined with other facial fractures. Fractures of the nasal bones and septal cartilage result in not only cosmetic deformity, but also functional disturbance. If early treatment is instituted, reduction and fixation is achieved properly, the disturbance of function can be prevented.
Management
Closed reduction is the treatment of choice for most nasal bone and/or septal fractures. These fractures should be repaired within 7 to 10 days. Closed reduction can be done under LA with or without sedation or general anaesthesia.
Mandibular Fractures (lower jaw)
Fractures of the mandible are common in patients, who sustain facial trauma.
Management of Mandibular Fractures in Adults
Closed Reduction
Most of the mandibular fractures can be treated by closed reduction. It is often advocated because of its relative simplicity, low cost and non-invasive nature of treatment. In closed reduction procedure, either dental wiring or arch bars are applied to individual dental arches and satisfactory occlusion is gained after reduction and IMF is carried out. The average recommended immobilization period for mandibular fractures is 6 weeks.
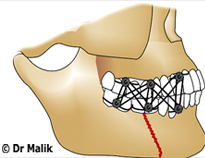
Open Reduction
Open reduction and rigid or stable fixation may be indicated as the procedure of first choice, when one or all of the following conditions are present:
- Displaced unfavorable fractures.
- Multiple fractures.
- Associated midface fractures.
- Associated condylar fractures.
- When IMF is contraindicated or not possible.
- To preclude the need for IMF for patient comfort.
- To facilitate the patient’s early return to work.
Bone Plating Advantages
- Rigid or stable fixation.
- Obviates the need for immobilization of the mandible.
- Early return to home and work.
- Soft diet can be taken.
- Maintenance of oral hygiene.
- Useful in mentally challenged, physically handicapped patients.
- Maintenance of airway in multiple fractures.
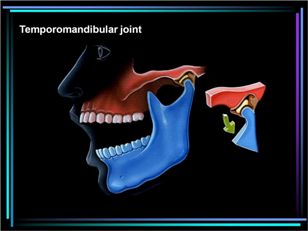
TEMPOROMANDIBULAR JOINT DISORDERS


TRISMUS:
Whenever, there is a restriction of normal oral opening or inability to open the mouth fully, the term trismus is used. Trismus is also defined as a condition in which muscle spasm or contracture prevents opening of the mouth (due to infection or other conditions which alter muscle structure).
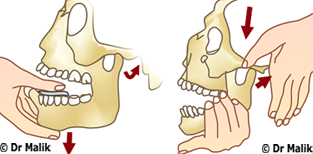
Dislocation, Subluxation, Hypermobility of TM Joint: The dislocation can be unilateral or bilateral.
Management
(i) reassuring the patient, (ii) tranquilizer or sedative drugs,
(iii) pressure and massage to the area, and (iv) manipulation.
Chronic Recurrent or Habitual Dislocation or Subluxation
The term is reserved for repeated episodes of dislocation, but the patient is able to manipulate it back into normal position. In such predisposed individuals, the acts of yawning, vomiting, laughing may precipitate subluxation.
Management
1. Intermaxillary fixation or limiting the oral opening by giving elastics Total immobilization of the jaw for the period of 3 to 4 weeks gives rest to the joint. But patient has to be kept on liquid diet. By applying prefabricated splint to the maxillary and
mandibular arches, elastic guidance can be given to restrict oral opening
2. Use of sclerosing solution injections into the joint space
The injection of this sclerosing solution brings about fibrosis in the
capsule, but the results are short-lived. Hence, the use is not recommended.Surgical management is also undertaken in severe cases.
Ankylosis of the Temporomandibular Joint and its Management Stiff joint:
Here because of immobility of the joint, the jaw function gets affected.Hypomobility to immobility of the joint can lead to inability to open the mouth from partial to complete.
Surgical Management
I :Condylectomy
II:Gap arthroplasty
III:Interpositional arthroplasty

Myofacial Pain Dysfunction Syndrome (MPDS)
Treatment of MPDS
First important task is counseling of the patient and giving the
assurance regarding prognosis and planning for symptomatic pain relief. Once the pain is relieved, then the patient’s acceptance for further treatment modalities is achieved
Behavior modification.
Modification of diet and home exercises should be suggested.
Initially soft diet should be prescribed along with the medication.
Physiotherapeutic Modalities
Heat application /Ultrasound /Ice packs /Massage with counter-irritants /Use of vapocoolent spray /Electrogalvanic stimulation /
transcutaneous electronic nerve stimulator (TENS)
Active stretch exercises
Each of these physiotherapy modalities can be very helpful to reduce the pain and increase the range of motion along with the medication.
Stress Management methods like acupressure, acupuncture, yoga, hypnosis, zen therapy, transcendental meditation, deep breathing relaxation, etc. also can help to relieve the stress.
Biofeedback instrument provides audio as well as visual output
allowing the patient to hear and see increased muscle activity and then relax.
Occlusal Splints are also fabricated to reduce spasm and disengage the teeth and create balance between the jaws and teeth.

ORTHOGNATIC SURGERY
Any deviation from the normal facial development definitely brings about an unpleasant facial appearance, with a disturbance in both aesthetics as well as function.
Types of Severe Skeletal Dentofacial Deformities
- Mandible Excess: Mandibular prognathism Deficiency:Mandibular retrognathism
- Maxilla Excess:Vertical maxillary excess(VME) Deficiency:Vertical maxillary deficiency(VMD)
- Combination
- Bimaxillary protrusion
- Nasomaxillary hypoplasia associated with prognathic mandible
- Nasomaxillary hypoplasia associated with cleft lip and palate
- Facial assymmetry:
- Asymmetric prognathism of the mandible
- Unilateral condylar hyperplasia
- Hemifacial hypertrophy (rare)
Severe Skeletal Dentofacial Deformities and Associated Problems
- Esthetic problems
- Functional problems
- Psychological problems (Tarnishing self-image)
- Impairment of mastication
- Impact on digestion—general health
- Associated speech problems
- Difficulty in maintaining oral hygiene
- Susceptibility to caries and periodontal problems
- Possible TM joint pain dysfunction.
Treatment
When a patient has got mild dentofacial deformities, it can be treated with orthodontic tooth movement alone. But, whenever there is severe skeletal dentofacial deformity exists, there are three broad options for treating these deformities.
- Growth modification
- Orthodontic camouflage
- Orthognathic surgery
Orthognathic Surgery
Orthognathic surgery includes surgical repositioning of the jaw and/or dentoalveolar segments. This option is used for the correction of a severe skeletal discrepancy after growth has ceased. The objective of orthognathic surgery is to achieve best function, best esthetics and best stability, thereby enhance the personality and lifestyle and channel the patient into self-esteem. For the successful outcome of the orthognathic surgery, both orthodontist as well as oral and maxillofacial surgeons are equal partners.
| Phase I | Presurgical orthodontic correction of upper and lower incisor inclinations to their skeletal bases. |
| Phase II | Superior and forward repositioning of the maxilla by a LeFort I osteotomy with simultaneous mandibular push-back by a sagittal split osteotomy and clockwise rotation of the mandible. The maxillary superior repositioning will be by 8 to 10 mm and maxillary an- terior repositioning by 4 mm. The mandibular push back will be by about 5 mm. |
| Phase III | Postsurgical orthodontic detailing of the occlusion followed by retention. |

PREPROSTHETIC SURGERY
Preprosthetic surgery is carried out to reform/redesign soft/hard tissues, by eliminating biological hindrances to receive comfortable and stable prosthesis. Reform/redesign denture Bearing area to create an oral environment to support a functional prosthetic appliance.
Aims of Preprosthetic Surgery
- Provide adequate bony tissue support for the placement re- movable partial denture or complete denture. (optimum ridge, height and width and contour)
- Provide adequate soft tissue support. Optimum vestibular depth.
- Elimination of pre-existing bony deformities, e.g. tori, promi- nent mylohyoid ridge, genial tubercle.
- Correction of maxillary and mandibular ridge relationship.
- Elimination of pre-existing soft tissue deformities, e.g. epulis, flabby ridges, hyperplastic tissues.
- Relocation of frenal/muscle attachments.
- Relocation of mental nerve.
- Establishment of correct vestibular depth.

DISEASES OF THE SALIVARY GLANDS
Salivary Gland Dysfunction
Sialorrhoea or Ptyalism excessive salivation seen in affected patients. It can be mild, intermittent or continuous profuse drooling. It can cause severe drooling, choking and social embarrassment to the patient.
Suggested Surgical Treatment
- Submandibular gland resection.
- Transposition of parotid duct.
- Parotid duct ligation.
Xerostomia: This is a subjective sensation of a dry mouth. Treatment is conservative, maintenance of oral hygiene, use of sialagogues(pilocarpine), modification of medications in elderly patients may help to improve the condition.
Sialolithiasis: Sialolithiasis is the formation of sialolith (salivary calculi, salivary stone) in the salivary duct or the gland resulting in the obstruction of the salivary flow. Patients complain of pain and swelling during and after eating the food. The obstruction of the duct by the sialolith causes prevention of salivary flow and increased pressure producing the pain.
Management
- The smaller sialoliths, which are located peripherally near the ductal opening may be removed by manipulation. (Called milking the gland)
- Larger sialoliths are surgically removed.
- Sometimes, the stones, which are not impacted, may be ex- tracted through the intubation of the duct with fine soft plas-tic catheter and application of the suction to the tube.
- Multiple stones or stones in the gland require the removal of the gland.
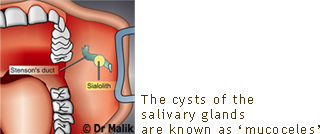
Mucocele
This is a swelling due to the accumulation of saliva, as a result of obstruction or trauma to the salivary gland ducts.
Clinical Features
Mucoceles occur as painless swellings, which may be recurrent. (Some patients give the history of increase in size during mealtime).
The common sites of occurrences of mucoceles, especially the extravasation type, are the lower lip and tongue, as they are the common sites for the trauma of the minor salivary glands. The retention type of mucocele is less common and rarely occurs in the lower lip. Instead, it occurs in palate, cheek, floor of the mouth and maxillary sinus.
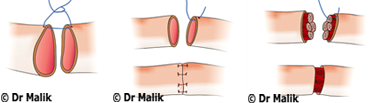
Treatment
Mucoceles are treated by surgical excision. It is common to see the recurrence after excision. It can be minimized, if the associated salivary gland acini are also removed.
Tumors of the Salivary Glands
The tumors of the salivary glands can affect the major and the minor glands. These tumors may be benign or malignant ones.
Treatment
Pleomorphic adenomas are treated by surgical excision. The parotid tumors are removed with adequate margins, whereas the intraoral lesions can be
treated little more conservatively. In case of submandibular tumors, excision of the gland with the tumor is performed.
Malignant Tumours
Mucoepidermoid carcinoma, adenoid cystic carcinoma, malignant mixed tumour, acinic cell carcinoma, is the common malignant tumours occurring in the salivary glands.
Management
- Debridement by hydrogen peroxide or saline
- Application of gentian violet
- The lesion is self-limiting one and heals in 6-8 weeks.
FACIAL NEUROPATHOLOGY/OROFACIAL REGION PAIN /SENSORY DISTURBANCES OF FACE AND JAWS
Injuries to peripheral branches of the fifth (trigeminal) nerve is ever-present risk during surgical procedures performed in the oral cavity and associated maxillofacial region. Sensory disturbances of the face due to trigeminal nerve branches injury usually undergo spontaneous regeneration and sensory recovery, but some will result in incomplete regeneration with paresthesia or will result in a painful neuropathy- dysesthesia
Management
Nerve regeneration in bony canals frequently occurs without surgical aid because the canal acts as a guide to growth and union.But if the bony canal is obstructed by displaced bone or a fragment of a tooth or soft tissue/muscle interposition, then the nerve regeneration is not possible without surgical intervention.
- i.Neurorrhaphy should not be performed until infection has sub-sided.
- ii.All pathologic conditions of the nerve ends must be resected (neuromas)
- iii.The nerve must be properly coopted.
Indications for Microneurosurgery
- Observed nerve severance.
- Total anaesthesia beyond 3 months.
- Dysesthesia beyond 4 months.
- Severe hypoesthesia without improvement beyond 4 months.
Contraindications for Microneurosurgery
- Central neuropathic pain.
- Dysesthesia not abolished by LA nerve block.
- Improving sensation.
- Sensory deficit acceptable to the patient.
- Metabolic neuropathy.
- Medially compromised patient.
- Excessive delay after injury.
CLEFT LIP AND CLEFT PALATE MANAGEMENT
The orofacial clefts are congenital deformities, which manifest at birth. Any disturbance during the embryological formation and development and growth of orofacial region will result in the formation of orofacial clefts. Orofacial clefts are the most frequently occurring craniofacial birth defects.
The zones affected by common orofacial clefts are as follows:
- Upper lip
- Alveolar ridge
- Hard palate
- Soft palate
- Nose (not so common)
- Eyes (not so common).
Management of Cleft Lip and Palate is done to
- To correct the birth defect surgically, so that patient can have acceptable facial aesthetics.
- To permit intelligible speech.
- To correct the dentition to allow normal function and aesthetics
General Management Protocol for the Cleft Patient
- Immediately after the birth—paediatric cosultation, counsel- ling, feeding instructions, evaluation by geneticist to decide whether it is an isolated cleft or if the cleft is part of the syn- drome, diagnosis of life expectancy of a child and diagnostic tests
- Within first few weeks of life—team evaluation, including hearing testing
- At 10 to 12 weeks—surgical repair of the lip, 3-6 months in India
- Before age 1 year to18 months—team evaluation and surgical repair of cleft palate and placement of pressure equalization tubes
- Three months after palate repair—team evaluation for speech and language assessment
- Three to six years—team evaluation—Medical, behavioural intervention as needed. Speech therapy, treatment for middle ear infection, fistula repair, soft palate lengthening, psycho-logical evaluation
- Five to six years—lip, nose revision if necessary. Pharyngeal surgery
- At seven years—Orthodontic treatment phase I
- Nine to eleven years—pre alveolar bone grafting
- Twelve years or later—Full orthodontic treatment phase II
- Fifteen to eighteen years—at the end of orthodontic treatment, placement of implants, fixed bridge, etc. for missing teeth
- Eighteen to twenty-one years—when most of growth is completed. Surgical advancement of maxilla, if required
- Final nose and lip revision—rhinoplasty, 16-18 years

Management of Cleft Lip/Timing of the Lip Surgery
The timing of the lip repair in infancy varies from first 48 hours of life to 6 months of age, depending on the surgeon’s judgement. 10 weeks of age with 10 gm of Hb and 10 pounds of weight. The trend is shifting toward early repair.

ORAL CANCER
The oral cavity is the most predominant location in the head and neck region for primary malignant tumours. The malignant tumours of the oral cavity can arise from either mesenchymal or epithelial tissues. Squamous cell carcinoma can arise from oral epithelium itself and from the terminal portions of the ducts of the salivary glands, minor and major. Salivary tumours arise from the minor salivary glands. Malignant melanoma arises from the melanocytes distributed in the basal layer of the oral epithelium.
Sarcoma can arise from cartilage, bone, muscle, fibrous tissue and fat (osteosarcoma, chondroma, chondrosarcoma). Lymphoma also occurs in and around the mouth.
The term “Oral Cancer” is nearly synonymous with squamous cell carcinoma, because of its predominance seen in the oral cavity. In all primary oral malignant tumours, 92% are the squamous cell carcinomas.
CAUSES- tobacco, alcohol, viruses, poor oral hygiene, constant trauma to mucosa due to dental cause
Premalignant Lesion
A morphologically altered tissue in which a cancer is more likely tooccur than in its apparently normal counterpart, e.g. leukoplakia, erythroplakia, erythroleukoplakia, erosive lichen planus.
1) Leukoplakia: A predominantly white lesion of the oral mucosa, which cannot be rubbed or dislodged or scraped off easily, and that cannot be characterized.
Treatment of Leukoplakia
- Removal of offending agent
- Stop use of tobacco, alcohol, etc.
- Attention to sharp teeth and ill-fitting dentures
- Chemo prevention.
- Surgical management- This can be accomplished either with conventional surgical methods (knife, electro cautery) or with the use of a carbon dioxide laser.
2) Erythroplakia: Red patches or plaques that cannot be characterized clinically or pathologically as any other definable lesion.
3) Oral Submucous Fibrosis (OSMF) It is a chronic progressive disorder and its clinical presentation depends on the stage of the disease at detection. The pathogenesis has been attributed primarily to the use of areca nut, the risk increasing with the duration and amount of its use. The majority of patients present with an intolerance to spicy food, rigidity of lip, tongue and palate leading to varying degrees of limitation of mouth opening (trismus).
Management of OSMF
Nonsurgical measures like local steroids, hyaluronidase injections, vitamin supplements have poor results. In the trismus, surgical release of fibrous bands in the oral mucosa and temporalis muscle myotomy may be performed. However, surgical procedures only partially relieve the trismus and do not have an effect on the underlying pathology. Therefore, as in the management of leukoplakia, aggressive counseling needs to be done with regards the cessation of areca nut consumption.
Management of oral cancers/malignancies
Treatment of oral cancer requires a team comprising of oncosurgeons, radiotherapists, and medical oncologists. In addition to these, supportive specialities such as radiology, pathology, speech therapy, dental and physiotherapy play an equally important and critical role.
Treatment of oral cancer depends upon the stage of cancer at diagnosis.
The broad guidelines are as follows:
Early stage oral cancer (Stage I and II) can be treated with single modality treatment.
Locally advanced and operable cancers (Stage III and IVA) need to be treated with combined modality treatment.Locally advanced, inoperable cancers or metastatic cancers (Stage IV B and IV C) are treated with palliative intent (Radiotherapy-RT or Chemotherapy-CT) or only symptomatic treatment if the patient’s performance status is low.
Advantages of Surgery
- Simple
- Fast
- No significant cosmetic and functional defects
- Repeated procedures possible
- Cost effective
Disadvantages of Radiotherapy
- Prolonged treatment
- Significant side effects like xerostomia, dental caries, osteoradionecrosis
- Can usually be given only once
- Not suitable for treatment if lesion involves or is close to the bone
Radiotherapy in Early Oral Cavity Cancer
Radiotherapy can be given either as brachytherapy) or as external beam radiotherapy. External beam radiotherapy is given with radiation sources external to the patient. Telecobalt machines emitting gamma rays or linear accelerators producing photons are commonly used.
Brachytherapy
In this form of radiotherapy, radiation is administered interstitially through catheters surgically placed across the lesion. Brachytherapy spares normal tissues such as bone, salivary glands and spinal cord. The ideal lesions suitable for brachytherapy should be less than 3 cm, superficially invasive and not close to the bone.

<Back to Top>

We are a family practice with 3 specialists covering the entire spectrum of your dental needs. Our philosophy is based on the concept of providing our patients with a comprehensive plan for ideal dental care

 Follow Us On
Follow Us On



